At the beginning of the month of April 2014 were the most newspapers in America talking about the arrival of the mysterious virus Middle East.
http://www.usatoday.com/story/news/nation/2014/05/04/indiana-mers-virus-health/8685487/
But, are you supposed to Americans fear the deadly syndrome the Middle East?
The Middle East respiratory syndrome coronavirus (MERS-CoV), also termed EMC/2012 (HCoV-EMC/2012), is positive-sense, single-stranded RNA novel species of the genus Betacoronavirus.
Respiratory disease definition is simply a disease affecting the human respiratory system and this of course includes lung illness by viral diseases.
There is no vaccine or treatment yet and any medical care is supportive and to help relieve symptoms. But CDC is discussing with partners the possibility of developing a vaccine.
What does that means?
What is the size of the risks that can be caused by a virus Corona respiratory disease?
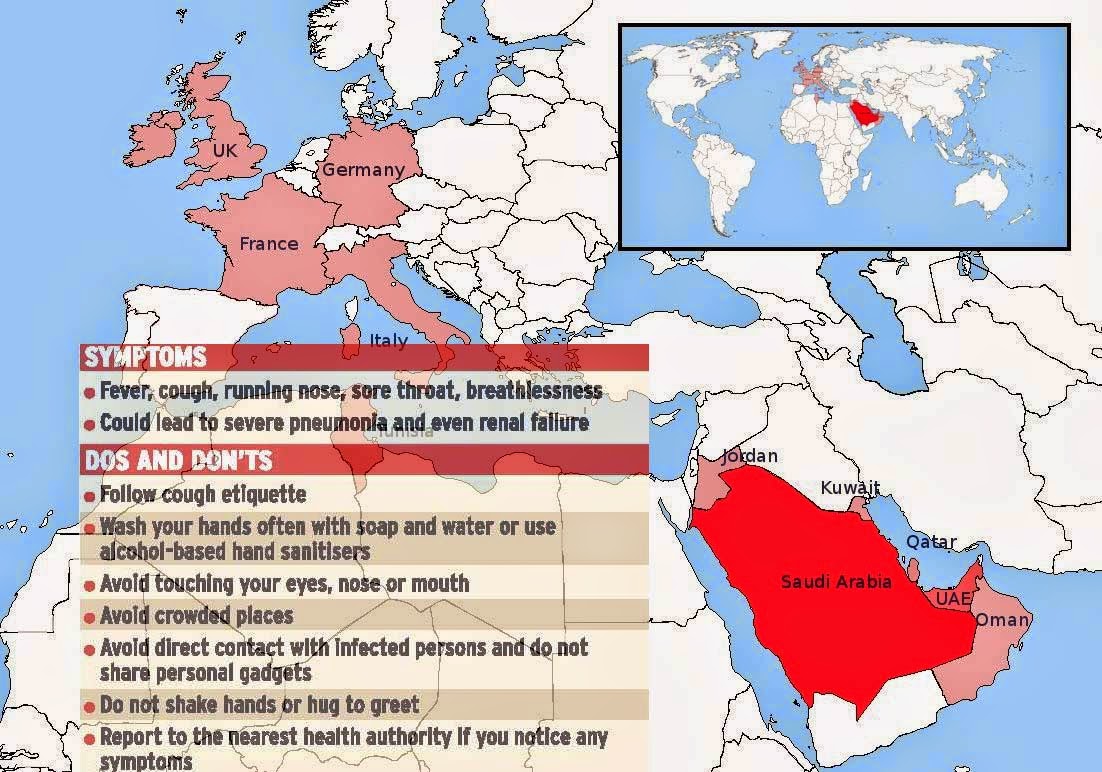
The official WHO MERS count is 238, with 92 deaths. As of 27 April 2014, there are 339 confirmed cases in Saudi Arabia, with 102 deaths. The first case of MERS-Cov in the United States was reported in Indiana on 2 May 2014.
There is very limited information on transmission, severity and clinical impact with only a small number of cases reported thus far.
Symptoms of Middle East respiratory disease: Most people who got infected with MERS-CoV developed severe acute respiratory illness with symptoms of fever, cough, and shortness of breath. 30% of them died. Some people were reported as having a mild respiratory illness.
Does respiratory diseases Coronavirus and SARS are the same?MERS-CoV is not the same coronavirus that caused severe acute respiratory syndrome (SARS) in 2003. However, like the SARS virus, MERS-CoV is most similar to coronaviruses found in bats. CDC is still learning about MERS.
The virus MERS-CoV is a new member of the beta group of coronavirus, Betacoronavirus, lineage C. MERS-CoV genomes are phylogenetically classified into twoclades, clade A and B. The earliest cases of MERS were of clade A clusters (EMC/2012 and Jordan-N3/2012), and new cases are genetically distinct (clade B).
MERS-CoV is distinct from SARS and distinct from the common-cold coronavirus and known endemic human betacoronaviruses HCoV-OC43 and HCoV-HKU1. Until 23 May 2013, MERS-CoV had frequently been referred to as a SARS-like virus, or simply the novel coronavirus, and early it was referred to colloquially on messageboards as the "Saudi SARS".
It is not certain whether the infections are the result of a single zoonotic event with subsequent human-to-human transmission, or if the multiple geographic sites of infection represent multiple zoonotic events from a common unknown source.
In humans, the virus has a strong tropism for nonciliated bronchial epithelial cells, and it has been shown to effectively evade the innate immune responses and antagonize interferon (IFN) production in these cells. This tropism is unique in that most respiratory viruses target ciliated cells
How to diagnose Coronavirus respiratory disease?How can you know that you are MERS Coronavirus infected?
What are the Laboratory tests to differentiate Coronavirus from other respiratory diseases?
What test should I do to investigate MERS coronavirus?
There are a limited number of commercial tests available, but these are not FDA-approved.
MERS-CoV is clinically diagnosed by taking nasopharyngeal swab examination and PCR for Coronavirus "MERS CoV PCR".
List of Specimens suitable for MERS-CoV testing based on current evidence by WHO:Specimens that do not need transport medium and should transport to laboratory in 4 degree C and shipped in cold ice if shipping was for more than 48 hours.
Serum for serological testing: paired samples are preferable with the initial sample collected in the first week of illness and the second collected two to three weeks later. A single serum sample should be collected at least 14 days after onset of symptoms.
Sputum, Bronchoalveolar lavage, tracheal aspirate, and nasopharyngeal aspirate.
Specimens require virus transport medium or sterile saline if specimen is also for bacterial culture. Combined nasopharyngeal/oropharyngeal swabs, tissue from biopsy or autopsy including lung
Interpretation of MERS-CoV test results and sensitivity:What does Positive MERS Cov Pcr test means?
Routine confirmation of cases of MERS respiratory disease infection is based on detection of unique sequences of viral RNA by real-time reverse-transcription polymerase chain reaction (rRT-PCR) with confirmation by nucleic acid sequencing when necessary. See below for a discussion of serological testing for MERS-CoV.
Suspected MERS virus must follow these steps by PCR test:
1- upE specific "rRT-PCR" .
2- If Positive, do "ORF 1a rRT-PCR" assay.
3- If Positive then the case is confirmed.
*rRT-PCR" means "real-time reverse-transcription polymerase chain reaction".
From WHO advices for May, 2014, for the potential infected people even if an initial test on a nasopharyngeal swab is negative. Repeat testing should be done when the initial testing is negative, preferably on specimens from the lower respiratory tract.
Investigation into the source of exposure should promptly be initiated to identify the mode of exposure, so that further transmission of the virus can be prevented.
In addition, the US Centers for Disease Control and Prevention (US CDC) has developed rRT-PCR assays targeting the MERS-CoV nucleocapsid (N) protein gene, which can complement upE and ORF 1a assays for screening and confirmation.
What should healthcare providers and health departments do?What should I do if I feel I am infected with Middle East respiratory disease?
The Last Update from WHO advice for respiratory disease infected people upon May, 2014:
1- Health-care facilities that provide for patients suspected or confirmed to be infected with MERS-CoV infection should take appropriate measures to decrease the risk of transmission of the virus from an infected patient to other patients.
2- It is not always possible to identify patients with MERS-CoV early because some have mild or unusual symptoms. For this reason, it is important that health-care workers apply standard precautions consistently with all patients – regardless of their diagnosis – in all work practices all the time.
3- All patients with symptoms of acute respiratory infection must have contact precautions and eye protection should be added when caring for probable or confirmed cases of MERS-CoV infection. Airborne precautions should be applied when performing aerosol generating procedures.
4- Recent travelers returning from the Middle East who develop SARI should be tested for MERS-CoV as advised in the current surveillance recommendations.
5- All Member States are reminded to promptly assess and notify WHO of any new cases.
6- People at high risk of severe disease due to MERS-CoV should avoid close contact with animals when visiting farms or barn areas where the virus is known to be potentially circulating. For the general public, when visiting a farm or a barn, general hygiene measures, such as regular hand washing before and after touching animals, avoiding contact with sick animals, and following food hygiene practices, should be adhered to.
